Sunil Dolwani, Dana Knoyle and Naomi Davies
A Challenging landscape
Colonoscopy is used to diagnose conditions such as colorectal cancer (CRC), inflammatory bowel disease and pre-cancerous conditions such as bowel polyps. However, it is an invasive procedure with significant demand on service and operator resources, time and length of time to achieve competence and expertise. Prior to the COVID-19 pandemic, the numbers of patients referred for endoscopy exceeded capacity across NHS Wales significantly, particularly colonoscopy. This situation has worsened and patients in Wales currently face long waiting times for diagnostic procedures such as Colonoscopy, leading to poorer outcomes. Significant workforce pressures and marked variation exists between health boards in diagnostic capacity and clinical expertise.
Innovation
“Every once in a while, a new technology, an old problem, and a big idea turn into an innovation.” Dean Kamen
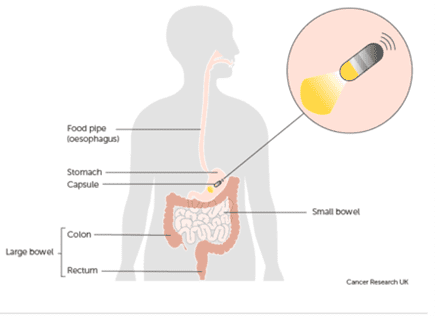
Colon Capsule Endoscopy (CCE) could contribute to solutions to colonoscopy capacity issues within the lower gastro-intestinal cancer pathway, by providing another diagnostic option for clinicians to offer patients waiting for a colonoscopy. We therefore planned to initiate, support and evaluate a pilot of CCE in 4 health boards in Wales, supported by the Bevan Commission Planned Care Innovation Programme and funded by Welsh Government.
Our aim was to:
- Support health boards to establish CCE services for patients in the lower GI pathway and explore translation of initial pilots into sustainable pathways.
- Pilot CCE as a novel intervention to explore its potential impact on workforce pressures across clinical roles and health board geographical and demographic boundaries.
- Collect, compare and analyse meaningful data to inform service pathways and associated patient outcomes as well as the impact on the service.
- Evaluate an All-Wales Information Governance model to enable equitable, efficient and safe diagnostic procedures for patients undergoing CCE.
- Trial a new national model of working that enables cross health board reporting to help with workforce pressures.
- Improve patient experience.

Did it work?
It was quite challenging to get going, but in the first fifty procedures:
- 8o% of patients had adequate bowel prep
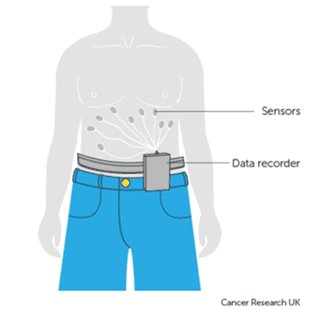
- 69% of patients completed the procedure (most common reason if incomplete – removing the sensor belt too soon)
- 57% significant bowel disease detected (IBD/polyps/cancer/diverticulae/haemorrhoids)
- Actions following CCE:
- Discharge to GP – 21%
- Back to referrer/secondary care – 17%
- Follow-up in clinic – 12%
- Further investigation – 36%
- There is demonstrable potential for impact on Colonoscopy demand and workforce pressures.
- The remote reader has demonstrated the feasibility of remote cross-health board reporting.
- 4 health boards have now established quality assutred colon capsule services in the pilot.
- There were challenges with information governance, cross-health board working and contractual issues.
What did we learn?
“Innovation is the ability to see change as an opportunity – not a threat.” Steve Jobs
We learnt that within the health service community in Wales there remains an enthusiasm for adoption of new innovation that might help our patients and services. This is despite the enormous pressures that colleagues face every day. However, this enthusiasm is in danger of tipping over into frustration if we don’t support these new innovations as opportunities to sustainably improve patient experience as well as development of our workforce and services and use these as catalysts to drive further evidence based change in our NHS (the training and skills development supported by the pilot would be lost if not used as a basis for further improvement).
We also learnt that selecting the appropriate patients through careful planning and analysis is more likely to give us good results and outcomes (or as Thomas Edison who invented the light bulb put it, “The value of an idea lies in the using of it.”). If we adopt an efficient Once for Wales approach (standardised evidence based criteria and quality assurance) then we can do much more as a team rather than fragmenting our efforts into smaller areas that worsen rather than reduce variation. We therefore need to see the change in colon capsule capacity embedded into the service and not just as a headline (Support the change not just the technology – Health Foundation). Like most good innovation this pilot has led us to reflect on wider aspects such as the significant advantages an All Wales model of staff contracts and Information Governance processes might give us. Now, that would be a future to aim for and combine our efforts towards.
The NEP Pathways team – Sunil Dolwani, Dana Knoyle and Naomi Davies.