Written by Dr Daryl Harris, Consultant Clinical Psychologist & Bevan Fellow.
The NHS is sick, some would say its dying. Yesterday’s solutions for the Service’s ills are failing to revive the vital signs of public and staff confidence. Continuing to do the same thing and expecting different results would be Einstein’s definition of madness. It is clear that we need to enact new remedies. But there is a catch. This paper argues that new ways of doing, first of all necessitate new ways of thinking. To quote a valued colleague, the key message is that we need to do the thinking, before we think the doing. But what do we need to think about?
Getting Under the Bonnet of Prudent Healthcare
My first car was a little Fiat 126. Small, efficient, and effective. Now with a growing family and a dog, the 126 is no longer fit for purpose. When the NHS was established, the main challenge was infectious disease and prescribing medication to passive patients was efficient, effective, and manageable. Now with people living longer the NHS has become a victim of its own success. We see a growing number of people struggling with long term conditions and multimorbidity, and treating people as passive patients to be fixed is no longer fit for purpose.
When I changed my car, I didn’t just switch to an updated Fiat 126 with a slightly faster and more efficient engine, I changed the make and model completely to meet my different needs. With climate change, I might now even question whether a car is the answer at all. Similarly, the kind of change we need in healthcare is not just about doing the same thing a bit quicker, more effectively, or with greater efficiency. Its about rethinking what is needed and reimagining how best to achieve this.
This paper challenges not just ‘the system’, but each of us working in the NHS to look under the bonnet of healthcare at the principles, beliefs, and values underpinning our practice. In so doing we need to look deeper than the possibilities of a bigger engine or a different model of car as this will only offer new choices about how we get from A-Z. Instead, we need to start by thinking again about what we mean by health and how this relates to healthcare and to also ask ourselves what our responsibility is in helping to make the changes. This should then offer new ways of thinking about the how, where, what, when, who, and start to provide a ‘route map’ for the journey.
We need new thinking to solve old problems
In 2015 the Bevan Commission launched a set of four principles for prudent health care. In short these are: co-production, prioritising those with the greatest need, using all skills to best effect, doing only what is needed, and reducing inappropriate variation.
These principles have been endorsed by successive Welsh Government Minister’s for Health and Social Care and now underpin Welsh healthcare policy.
Having these principles without translating them into practice will achieve nothing. So will seeing them simply as a set of actions to be done without changing our underlying thinking. Co-production, triage, providing the minimum that is needed, and carrying out evidence-based practice can all be done in a way that is still driven by existing expectations, values, and beliefs, even if these represent the same thinking that has led the NHS to the current point of existential crisis. Whilst these habits of thinking lie under the surface, unacknowledged and unexamined they will continue to form the hidden hand guiding (and limiting) healthcare practices and innovation. As Einstein famously said, “We can’t solve problems using the same kind of thinking as when we created them”.
This paper respectfully suggests that the kinds of changes required to support prudent health and care and create sustainable health and care services need to start with a process of self-change for the people working in these services. In his short book Teaching Smart People to Learn, Chris Argyris distinguishes between single and double loop learning. The former involves looking outwards to identify efficiencies and improvements that can be made to organisational structures, processes, roles, and behaviours. This is the kind of development that is driven by continuous improvement initiatives. This incremental change is of course of value. However, Argyris notes that it has its limits. Notably it tends to drive a focus on changing other people. This is because single loop learning does not encourage or support people to look inwards. In contrast, double loop learning requires reflection on the principles, assumptions, and values underpinning healthcare practice. Left unexamined, these principles not only determine the limits of current practice, but also of future models of practice.
Moving beyond the Zoom and gloom
In a 2021 the Department of Health and Social Care in England[1] published a study which focussed on the problem of over prescribing. In this study, the public reported that they did not feel listened to and as a result the prescription they received did not address their issues or preferences. Interestingly, in the same study practitioners reported often feeling like they had not got to the root of the person’s problems, and as a result the treatment they offered was dealing more with the symptoms than the cause.
The overprescribing study highlights the close connection between the experience and needs of health care providers and recipients. Afterall, providers are also members of the community and take their turn as users of health services. This highlights the importance of embedding values, beliefs, and principles that are responsive to the needs of everyone participating and contributing to health care. The approach to the recovery of services after the covid pandemic is a good illustration. The message to practitioners seems to be something like, ‘thank you for your efforts during the pandemic, but for now you need to run a little faster and a little longer so we can recover the functioning of our services’.
Focussing covid recovery on the re-establishment of previous functioning parallels the traditional view of ‘clinical recovery’ as the restitution of function. The aim being to return as near as possible to the premorbid state. This curative model worked well in the era of treating transmissible diseases. As the focus of healthcare shifts more and more to multiple and long-term conditions it is proving less helpful. Arguably, one of the consequences is the burgeoning demand on services and the resulting public dissatisfaction and staff burnout.
An alternative way of thinking about recovery was provided by William Anthony in 1993[2]. His description of ‘personal recovery’ is as a “deeply personal unique process of changing one’s attitudes, values, feelings, goals, skills, and roles. It is a way of living a satisfying, hopeful, and contributing life, even within limitations caused by illness”. Translating this into a service context, recovery of services from covid could be seen as a process of change in the attitudes, values, feelings, goals, skills, and roles underpinning practice so that both service recipients and providers can live (and work) as well as possible within the constraints imposed by current resources, finances etc.
In contrast to ‘clinical recovery’ which seems to focus on what Chris Argyris describes as single loop learning, the very nature of personal recovery necessitates a process of self-reflection which feeds double loop learning. The suggestion has already been made that this in turn opens-up new and previously unforeseen opportunities for growth, development, and transformation rather than dissatisfaction and burnout.
The two approaches to recovery parallel two different narratives of the pandemic. Clinical recovery leans into the story of the medical frontline in saving sick people. The efforts of this front-line were herculean. The accomplishments of staff from health and social care in sustaining patient’s bodies, minds and spirits are deserving of every gratitude.
Although barriers to medical care during the pandemic clearly had a negative impact for some people, the flip side is that communities showed incredible ingenuity and resilience in supporting the health and wellbeing of their members. The colossal community effort brought people and communities closer, despite the physical restrictions of social distancing. This is the second story of the pandemic. This is the story of how the people of Wales underwent a deeply personal unique process of changing their attitudes, values, feelings, goals, skills, and roles to enable satisfying, hopeful, and contributing lives, within the limitations imposed by the corona virus pandemic and associated public health measures.
Stepping on the toes of ‘bare foot medicine’
Ivan Illich coins the phrase ‘barefoot medicine’ as a way of describing the efforts of non-medically trained members of the community to support health[3]. It is from the spirit of ‘barefoot medicine’ that the NHS was born. In 2022 the Bevan Commission published an article written by Paul Buss. The article was titled “Values to value” for recovery and renewal: Putting Prudent Healthcare into practice. With respect to the collective values underpinning the NHS in Wales this article highlighted the roots in our local communities and the founding principles of community, collective responsibility and caring for each other. Paul Buss rightly links these values with “a strong history established through Aneurin Bevan of a sense of fairness, equity and equal opportunity in order to enhance health and well-being and that of future generations”.
Aneurin Bevan learnt these values in his hometown of Tredegar. The miners and steelworkers of the town, including my grandfather, voluntarily paid a proportion of their meagre wages into a community fund that ensured free healthcare at the point of need. They paid additional money and volunteered time to support the various welfare societies and miners’ institutes. These institutes focused on self-improvement, peer support, and co-operation. Outside of their hard physical labour, they provided workers and their families with a sense of connection, community, meaning, purpose, recreation, status, creativity, and hope. Research has shown that these are the human needs that allow people to live well[4] – both then and now.
Although things are now better in so many ways, there seem to be important lessons from the past that services have forgotten.
Lesson one is that the duties of care that people hold for themselves and each other are paramount, and that the role of state services is to catalyse and nurture citizens’ ability to look after their own health and that of the people around them. Not to do it all for them. The exception being circumstances where proximal sources of support are unable to address an imminent, significant, and foreseeable risk to wellbeing.
Lesson two from the past is that health is not the opposite of illness, it is the ability to follow valued life plans underpinned by shared human needs for wellbeing.
These two lessons have relevance to the recovery of health services following the pandemic. The incredible resilience and resourcefulness shown by the community during the pandemic raises questions about whether health care professionals and policy makers are underestimating the community’s potential to look after itself. The sense of value and wellbeing people experienced through their efforts to support and look after each other raises additional questions about the risk that underestimating a community’s health capabilities poses to its wellbeing.
The above considerations regarding covid recovery point to the critical importance of decisions about when and when not to intervene. This brings us to the heart of prudent healthcare. The intimate links between prudent health care and prudent decision making have been highlighted by Kate Malcomess the author of the Care Aims Intended Outcomes Framework[5]. This framework emphasises the foreseeable impact on the person’s life plan as the basis for decisions about preventing harm – making risk judgments personal and meaningful. It also requires practitioners to use a staged approach to risk management with a strong emphasis on building capacity in the person, family, and the people around the family, avoiding dependency. Services adopting the Care Aims principles have found that this emphasis on prevention, early intervention, and capacity building both in the population and in the community of practitioners, supports reductions in unplanned admissions, length of stay, and avoidable readmissions.
Guests in people’s lives, not hosts in our care-systems6
Much has changed since the era of Aneurin Bevan. Coal is no longer fashionable. It can no longer be thought of as black gold. Carbon is a dirty word. But an interesting thing about carbon is that the form it takes and the impact it has depends largely on the conditions with which it is treated. What is true of carbon is also true of people. Arguably the way service providers have learnt to treat and engage with service recipients does not maximise their ability to shine.
In 2016, the Bevan Commission suggested that “Implicit in a prudent approach to health is the need to redraw the relationship between citizen and the state, so that professionals and the public can work together as equal partners; co-producing new services that best fit their needs and empowering people to gain greater control over their own lives”[7]. It seems clear that with ever increasing demand, shrinking resources, increased public dissatisfaction, and faltering morale in public servants – now more than ever – there is a need to make the vision of a revised contract between citizen and state a reality.
If service providers rely on single loop learning to guide the reworking of the healthcare contract there is a risk that they will focus on changes the public need to make. This may well have a detrimental impact on the quality of relationship, resulting in a hardening (rather than softening) of the boundary between provider and recipient. This is clearly against the hopes of practitioners, policy makers and the public. It is important that they remember they are the other half of the healthcare relationship and the other side of the service boundary. Another way to change both the relationship and boundary is through self-change, guided by a process of self-reflective double loop learning.
Changing the well-engrained beliefs and principles underpinning current practice is a challenge that is perhaps as profound as that needed to support decarbonisation or to turn coal into diamonds. The beliefs sustaining old coal fired health care systems include:
- A focus on problems that are localised within individuals.
- Reliance on professionals as the main source of expertise.
- People being treated as patients who are passive recipients of healthcare.
- An emphasis on professionals as the active agents of change.
- A culture that continues to promote a power imbalance between service providers and recipients.
Single loop continuous improvement initiatives focus on trying to do these things better – i.e., on health professionals getting better at finding problems, developing their expertise, and enhancing their capacity to engineer clinical change. If the full potential of Prudent Healthcare is to be realised, efforts to do things better need to be matched or superseded by efforts to do better things. Things that are underpinned by new ways of thinking about their work. Ways of thinking that unearth diamonds and move past the production of coal.
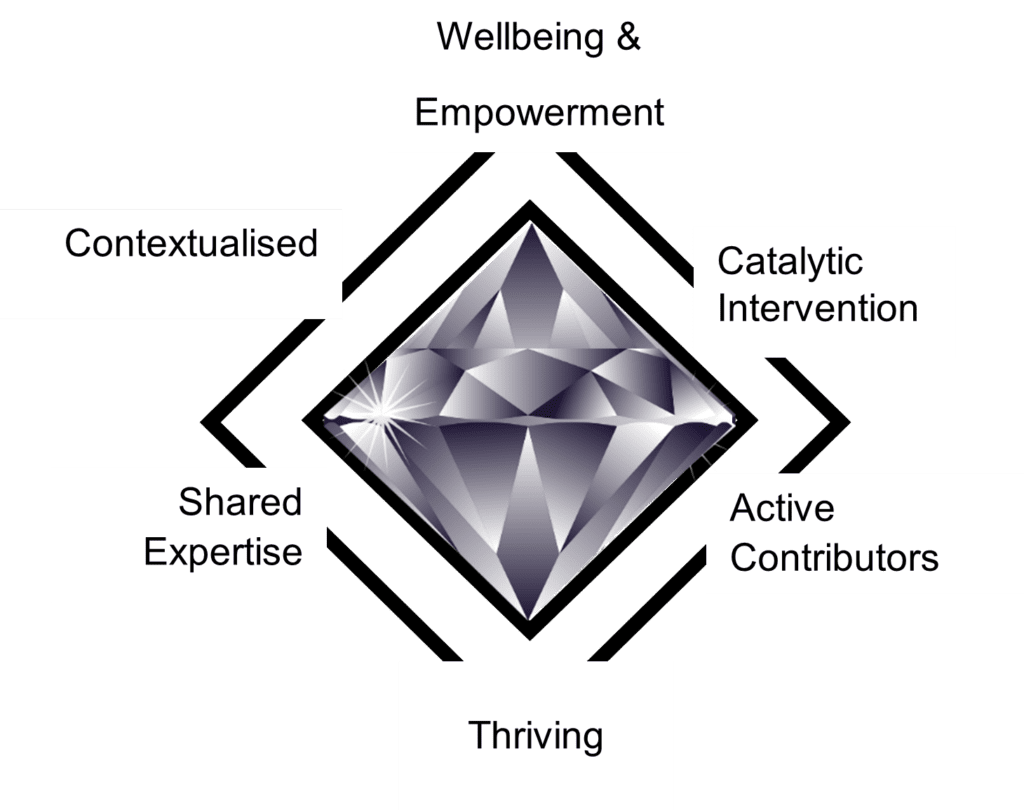
Examples of principles that might help to transform health and social care services in the direction of Prudent Health Care are summarised in Figure 1. These focus on:
- Wellbeing, hope, and control – rather than problems and deficits.
- The contextualisation of life challenges within people’s history, family, values, choices, culture, and community.
- Creating capable communities with professionals as the catalysts and not the agents of change.
- Shared expertise and the need for the prudent use of all skills, assets & resources, to achieve the greatest good, and
- Working in the citizen space[8] with everyone as active participants and equal partners in co-creating thriving communities.
Moving beyond petty lives to preserve the reasons for living
In his book ‘Being Mortal’, Atul Gwande highlights that for many, at the end of life the tragedy is not just dying, it is the manner of death[9]. He poignantly articulates how healthcare cannot just be about preserving life but must also be about preserving the reasons for living. This is a thread running through this paper. It also runs through the work of Kate Malcomess and the Care Aims decision-making framework she has developed[10]. Care Aims outlines the need for health care professionals to take the time to find out what matters to people, how they are making sense of current risks to these things, and what they see as being potentially helpful in addressing these risks.
In a parallel argument, leaders and change makers need to start by engaging with what matters to the people involved in a change. It is not enough to focus changes on increased efficiency, these changes also need to focus on maintaining or even enhancing the wellbeing of staff.
As an illustration, working with communities to catalyse and nurture their resilience and ability to make changes, rather than being the source of this change, requires healthcare workers to foreground citizen’s expertise and downplay their own. This has implications for the way health professionals meet their human needs for a sense of achievement, status, and purpose.
In a similar vein, focusing health care on building community capability and resilience suggests the need to rebalance the allocation of resources between the community of the hospital and the wider community. This has implications for the status of specialist and secondary care healthcare professionals. This needs to be considered in the way that specialist expertise is reorganised to support generalist-specialists in the community. Continuing to recognise the value of specialist knowledge but mobilising it to where it is needed to support colleagues in the community, rather than moving members of the public to where it is currently located in secondary care centres.
To make these and other changes, practitioners will need to find new ways of thinking that not only open the door to transformational change, but that also leave them feeling good when they pass through it. This will necessitate adjustment to not only what they value in their own minds but also the signals about value that are encoded in the way the system measures, reports, and rewards service activity. This means that the process of re-examining and updating the values, principles, and thinking underpinning healthcare needs to be system wide – extending beyond practitioners, to managers, leaders, boards, and policy makers.
The above raises an obvious question about whether the suggested changes in thinking are worth the effort. There is a statistic that 70% of change initiatives fail to meet their objectives. Whilst the validity of this statistic is questionable, it is clear to anyone working in health and social care that transformational change is illusive. This is illustrated by the stubborn challenge of integration within and between services.
This paper has suggested several potential reasons for the illusiveness of transformational change. It has also offered suggestions for how health services might overcome them. It has emphasised the need to focus inwards on self-change, starting with how practitioners, leaders, and policy makers think about their work, rather than focusing outwards on what they do or more frequently on what they expect other people to do. Failing to do so prevents reflection on the principles and values that constrain, but also give meaning to their current practice. Understanding and critically reflecting on these principles creates the freedom that allows service providers to think and act differently, but perhaps more importantly it opens the possibility for them to do this in a way that allows them to continue to feel good about their work.
In summary, some people repeatedly buy the updated model of the same car. This reflects an approach to learning that recognises the incremental benefits of doing similar things differently. This single loop of learning does not provide a sustainable model for healthcare transformation. This is because it leaves the beliefs and principles underpinning action unexplored. The Spanish philosopher Jose Ortega noted that “Our firmest convictions are apt to be the most suspect, they mark our limitations and our bounds. Life is a petty thing unless it is moved by the indomitable urge to extend its boundaries”. The boundaries of motoring have shifted with the change from carbon-based fuel to electric engines. Perhaps more importantly people are now questioning the need for and meaning of travel. Transforming healthcare will necessitate a similar change. To extend the metaphor, it will require service providers to not only experiment with changing the habits of thinking that currently sit under the bonnet of healthcare but also to reconsider the need for the bonnet, the engine, a car, and to consider alternative means of transport and the meaning of travel itself. In brief to rethink health and its relation to healthcare. Unchallenged, these habits of thinking provide the chains that bind health services to their existing practices, impeding transformational change.
The recent stretch of road has been a hard one, the next looks harder still. People are tired and the temperature gauge on the dashboard is flashing. It’s time for us all to stop. To look under the bonnet but also to have a good look around and within.
This brings us to the heart of the matter – the so what? What do we need to do to ensure that prudent health care succeeds in its ambition of creating sustainable services. In systems theory the beating of a butterfly’s wings on one continent can, via a series of interconnected events, lead to a tsunami on the other side of the world. Each of us needs to beat our metaphorical wings by committing to organisational change. Quinn and Sonenshein[11] outline four general strategies for this change. The commitment called for in this paper is not to either of the first two strategies described by Quinn and Sonenshein – telling or forcing others to change. Instead, it is for a commitment to participation and transformation.
Participation requires each of us to look outwards to change our external relationships. To reach out through dialogue and collective enquiry to align our best hopes with those of our colleagues, stakeholders, and communities. From inception, this process has been at the heart of health services in Wales born out of the recognition of our interdependency.
The second strategy requires us to look inwards to change our internal relationships between our values, beliefs, hopes and actions. In this transforming strategy the lever is personal integrity, which gives rise to what Quinn and Sonenshein refer to as moral power. They argue that through moral power, we are not presenting a single view of the good life. Quite the contrary, each of us needs to find their own moral power. This derives from reduced defensiveness, examination of personal hypocrisy, and commitment to a higher purpose such as universal health. This is akin to the concept of personal mastery outlined by Peter Senge in ‘The Fifth Discipline’[5]. This transforming strategy challenges each of us as change agents to explore how principled and congruent our beliefs, behaviours, values, interactions, and actions are with our stated aims.
This takes us back to Chris Argyris and the distinction between double and single loop learning. Simply put, a transformational change strategy requires us to be willing to look within to explore how we might currently be part of the problem as well as part of the solution. This requires organisations, managers, leaders, and communities to contribute to the creation of places and spaces for both recovery and discovery, making good on the promise and promises of reflective practice, mentoring, compassionate leadership etc. These are places that provide the psychological safety needed to enable changes in attitudes, values, feelings, goals, skills, and roles leading to the experience of satisfying, hopeful, and contributing lives and work lives within any limitations caused by illness or scarcity of resource.
As a final thought it is vital that leaders and managers also avail themselves of these places and spaces. This is to ensure close alignment between their espoused hopes, values, and beliefs, and the one’s that run under the surface forming the hidden hand that guides their actions. This is the same hidden hand that calls for practitioners to ‘act at the edge of their licence’ whilst at the same time tethering them to guidelines, governance, data capture, and targets that prescribe their decision making. This is not a call for abandoning the need for assurance, it is a call for unrelenting and honest self-reflection on the desired end and aligning our internal and external relationships in the service of this end.
Acknowledgements
The ideas presented in this paper owe a lot to the time I have spent working with Kate Malcomess and Jack Bush. Respectively, the creator of the Care Aims Intended Outcomes Framework, and Cognitive Self Change. They have also been shaped by my work with the ABUHB Acquired Brain Injury and Community Neuro Rehabilitation Services, by my involvement in the Bevan Commission Exemplar Programme, my work with Nick Andrews from the University of Swansea using the Most Significant Change Technique, and engaging discussions with Des Brown Q Lab Cymru Programme Lead Improvement Cymru.
References
[1] Good for you, good for us, good for everybody: A plan to reduce overprescribing to make patient care better, safer, support the NHS, and reduce carbon emissions. Department of Health and Social Care. 22 September 2021
[2] William Anthony (1993). Recovery from mental illness: the guiding vision of the mental health system in the 1990s. Psychological Rehabilitation Journal, 16(4), 11-23.
[3] Ivan Illich. (1974). Medical Nemesis: The Expropriation of Health. Calder & Boyars.
[4] Deci, E. & Ryan, R. (1985). Intrinsic Motivation and Self Determination in Human Behaviour.
[5] https://careaims.com
[6] Donald Berwick, (2014). Promising Care: How we can rescue health care by improving it. Jossey-Bass.
[7] https://bevancommission.org
[8] Cormac Russell, (2020). Rekindling Democracy: A professional’s guide to working in citizen space. Cascade Books.
[9] Atul Gwande, Being Mortal: Illness, medicine, and what matters in the end. Profile Books Ltd.
[10] Care aims reference or link to website
[11] Quinn, R.E., & Sonenshein, S. (2008). Four general strategies for affecting change in human systems. In T.G. Cummings (Ed.), Handbook of organization development (pp. 69-78). Thousand Oaks, CA: Sage.
[12] Peter Senge, 1990, The fifth discipline: The art and practice of the learning organization, by New York: Doubleday/Currency.