Karen Hazel
Aneurin Bevan University Health Board
The proposed project is building on lessons learnt from a successful collaborative service improvement piece of work between the Nurse – Led Heart Failure (HF) Service and the Value Based Health Care Programme within Aneurin Bevan University Health Board (ABUHB). Initial work to redesign the inpatient pathway for patients discharged from acute cardiology care resulted in a significant reduction in referral to appointment waiting times. In 2019/20 patients post hospital discharge were waiting an average of 63 days from receipt of referral to their first outpatient hospital appointment.
Since October 2020 all patients now have two appointments within 35 days. Timely follow up post hospital discharge allows optimisation of medications within four months which previously had taken up to 12 – 24 months. This is significant as it means that as a service, we are meeting both National audit and evidence based standards which historically we were unable to achieve.
Redesigning the pathway enabled the service to collect Patient Reported Outcome Measures (PROMs) to embed patient engagement at given points along the pathway. It soon became apparent that a large cohort of patients did not need an outpatient appointment within a secondary care setting.
Aims and Objectives:
- To test a different Model to reduce readmissions, increase cardiac rehab uptake and improve outcomes related to quality of life and health outcomes
- To place a greater emphasis on rehabilitation for delivering evidence-based programme of care and optimizing HF patients on their medications
- To free up specialist capacity for the more complex patients
Project Impact:


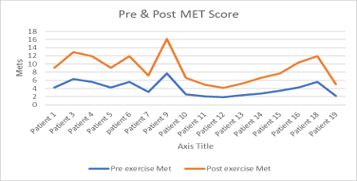
- Improvements in exercise, QOL – reporting reduction in anxiety and depression score.
- Optimisation of medication was achieved on average 15 weeks compared to 28 weeks in usual care.
- Readmission rate 1.5% ~ usual readmission rate 25%.
- 335 appointments were freed in secondary care for more complex patients.
- Co-Production Meetings x 3 held.
Patient Benefits:

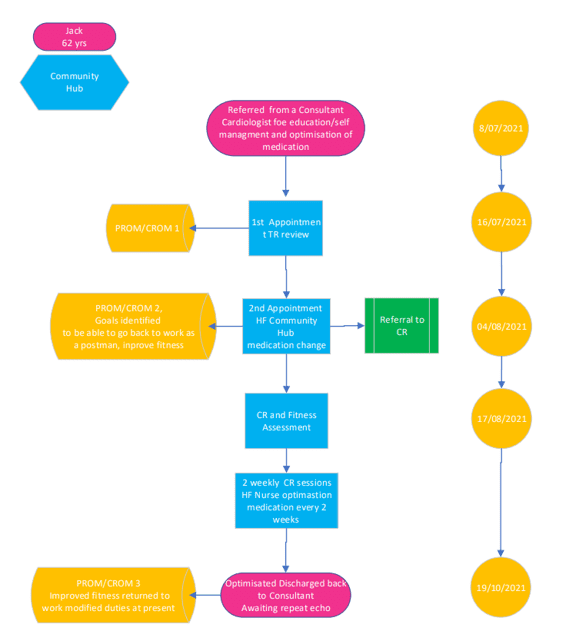
Joseph’s pathway reflects timely delays and numerous secondary care appointments. Lacked patient engagement.

Jack was seen timely, as per NICE/NICOR guidelines was optimised on treatment with 3 months. He was engaged in his care and his goal was achieved through attending Cardiac Rehabilitation.