Christine Sillman
Abertawe Bro Morgannwg University Health Board
This Bevan Exemplar project introduced a new role as a specialist Palliative Radiographer, to enable quicker and easier access to radiotherapy.
Background:
Patients with a diagnosis of metastatic (secondary) cancer may need palliative radiotherapy treatment to alleviate painful symptoms. These symptoms can be so severe that they affect quality of life, and a cancer patient may need emergency radiotherapy for very urgent conditions such as spinal cord compression.
The Royal College of Radiologists recommends that for urgent radiotherapy, good practice is to start treatment within 24 hours following agreement between clinician and patient, with 48 hours being the maximum acceptable delay. For palliative radiotherapy, good practice is recommended to be 2 days with a maximum delay of 14 days.
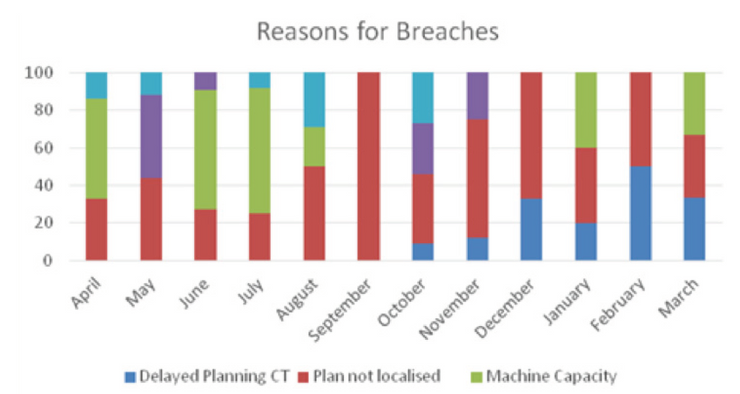
Patients waiting for palliative radiotherapy are often in considerable pain and if you can improve the pathway to treatment for them and hence improve symptoms more quickly, this could have a significant impact on their quality of life – every day counts when faced with an incurable illness. The team carried out an audit (April 2016 – March 2017) to reduce time to access palliative radiotherapy. The most common reasons for delay included machine capacity, machine breakdowns and a delay in planning and approval.
As a result of this study, ‘Reducing Time to Palliative Radiotherapy’ (Higgins, Banner, Sillman et al 2017), some improvement has already been achieved by enabling staff to use electronic planning, approval and prescribing systems remotely, however there were still delays due to the availability of already very busy clinicians to plan and approve palliative treatments on time.
Aims:
It was decided that there was scope to improve this service by better utilising the skills of highly trained and experienced radiographers, who have completed postgraduate-level study in relevant areas of practice.
The aim of the Bevan Exemplar project was to develop an advanced practice role as a specialist palliative radiographer, following completion of a mentorship programme working closely with Consultant Clinical Oncologists, in addition to having completed relevant Masters-level modules leading to an MSc in Professional Practice. Relevant modules included:
- Palliative radiotherapy planning;
- Informed consent;
- Cross sectional anatomy;
- Evidencing work based learning.
Challenges:
To achieve this aim, collaboration was key: the team worked with colleagues in other Cancer Centres who have Consultant or Advanced Practice Palliative radiographers already in post, or who are developing a similar role. A business plan was developed, with included protected time to spend shadowing Consultant Oncologist/Mentor in regular clinics, and for project work.
The new specialist Palliative Radiographer will be required to keep records of developing competencies, complete learning modules, attend specialist training sessions and secure both local and academic mentors to ensure they met the required standards for the role.
A radiographer- led clinic for palliative radiotherapy will run alongside a clinician- led clinic, and appropriate referrals will be diverted to the palliative radiographer for consultation, consent, planning, prescribing and approval of radiotherapy treatment.
Outcomes:
A major outcome of this project is that it will ensure quicker and easier access to palliative radiotherapy, by reducing the time taken for treatment planning and therefore reducing the delay for patients awaiting urgent treatment. It also enables busy clinicians to spend more time in planning radical treatments and therefore will have a ‘knock-on effect’ in reducing waiting times for all radiotherapy patients.
Next steps:
The foundations of the idea to set up this role have been ongoing for a number of years with obstacles delaying it – mainly staffing shortages. However, it is slowly being realised that this will ultimately result in a more efficient service and improved patient experience, and it is now progressing with awareness and support increasing all the time. It is the project lead’s aim to have the role up and running fully within the next six months.
“The link with the Bevan Commission has helped to promote this project and bring it to people’s attention.”
Christine Sillman, Therapeutic Radiographer

