Callum Mackay, John Glen and Ffyon Davies
Betsi Cadwaladr University Health Board
Background:
Ysbyty Glan Clwyd’s ICU currently samples multiple bottles of blood from each patient every day. While there are good reasons to repeat blood tests frequently in critically ill patients, our current practice of 10 – 11 standard blood tests requiring 4 blood bottles as performed each morning results in lots of tests that do not give us useful information or help guide treatment.
Blood tests are not completely without risks and harms, for example, increasing amounts of blood taken correlates well with both how many of our patients become anaemic and how many blood transfusions we administer each year.
These risks must be considered against the need for close monitoring, and ideally, each patient should have the blood tests they require each day considered on a case-by-case basis, to maximise benefit and prevent unnecessary harm.

Project Aims:
The primary aim of our project was to eliminate ‘standard’ blood tests orders and prompt all clinicians to consider the tests each patient requires each day.
With this system in place, we hope to see:
- Reduced rates of anaemia and improved patient outcomes.
- Reduced usage of blood transfusions.
- Reduced usage of consumable products and waste from unnecessary blood draws.
- Reduced costs of blood tests incurred by our blood sciences laboratory.
- Reduced need for painful, repeated blood tests and increased patient wellbeing.
Challenges:
COVID 19 has presented huge challenges to Intensive care units all over the world, and ours was no exception. Changing how we practice in the context, however prudent and necessary, was always going to be difficult.
The biggest hurdle to implementing this system has been in educating our large number of staff and maintaining their engagement with the new system. For patient safety, staff are instructed to order the full ‘standard’ set of blood tests if unsure or if no blood tests have been specified, so it’s vital everyone involved has access to training to ensure we continue only taking the blood tests we require.
Key Outcomes:
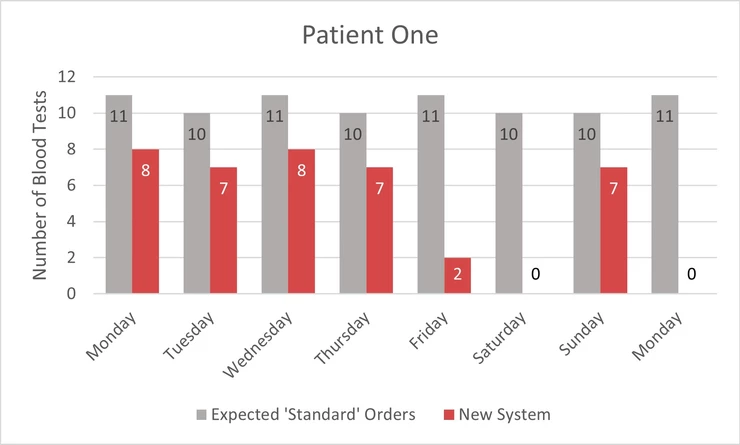
At time of writing, our system is freshly introduced into our ICU and detailed data collection is ongoing, but initial results are encouraging, and we’d like to share some examples of the new system in action, each graph below shows the number of blood tests ordered for each patient next to the ‘expected’ ordering under the old routine system.
Patient One
Patient One was admitted extremely unwell, and initially required multiple antibiotics and surgeries to control a life-threatening infection, we’re extremely pleased with his ongoing recovery now, and the blood tests ordered for him each day demonstrate more frequent, comprehensive testing as he was critically unwell, reducing as time and recovery progress.
Patient Two
Patient Two was admitted following a surgery that had resulted in complications, while he made a swift initial recovery, he went on to develop an infection and became increasingly unwell. His blood tests demonstrate how the new system allows us to respond to improving patients by reducing our monitoring of blood tests, and increase their intensity if needed.

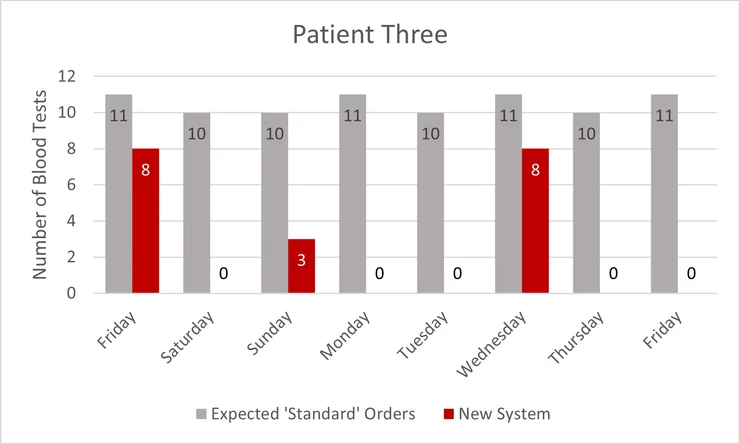
Patient Three
Patient Three is clinically stable, but she must remain in intensive care for advanced respiratory care. Her blood tests demonstrate how safe, periodic blood testing is used to reduce the burden of repeated blood tests over weeks and sometimes months.
During the review process, it was identified that three of the eleven standard order blood tests were often redundant or did not frequently change our clinical management, these three tests are now performed very infrequently.
Because of this change alone, we know that:
- We will order up to 11,000 fewer blood tests in the coming 12 months.
- This will lead to an approximate cost saving of £44,000 in laboratory consumables alone.
Next Steps:
We need to continue educating and supporting staff in the use of the new system as time goes on, to ensure that all opportunities to reduce the impact we have on our patients are captured.
We may also need to adapt the system, listen to feedback on its implementation and produce something that works well for all members of staff and allows easy adoption by other intensive care units.
Over the coming months, we plan to collect more data to answer the following questions:
- Can we quantify the average reduction in the volume of each blood draw?
- Can we more accurately quantify reduction in both blood tests and associated costs?
- Have we reduced our rate of blood transfusion?
- Have we had a negative or positive impact on staff workload and patient experience?
Our Exemplar Experience:
The Bevan Commission helped us understand and manage the process of changing our practice in a productive and inclusive manner.
Showcase:
Contact:
Callum MacKay: callum.mackay@wales.nhs.uk

