Carly Pridmore
Hywel Dda University Health Board
Background:
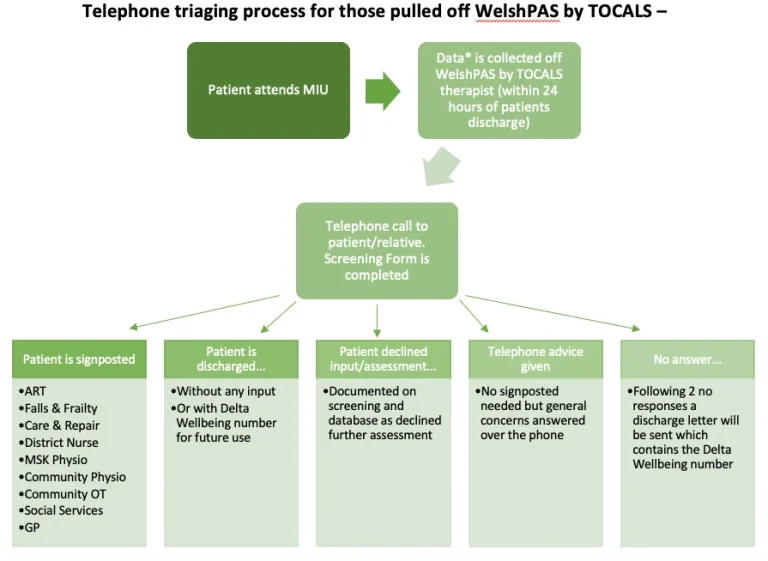
The Transfer of Care, Advice Liaison Service (TOCALS) provides a discharge service in the Minor Injuries Unit (MIU) in Prince Philip Hospital, Llanelli. Historically, Front of House (FOH) professionals were dependent on MIU staff to leave patient details for urgent therapy or Integrated Care Sister follow ups. These patients are then contacted and provided with either telephone advice/signposting or an urgent home visit if necessary.
Since COVID there have been service changes, high turnover of patients and staff shortages in MIU and these referral have reduced. The project was identified to begin a more in-depth screening process where FOH staff identified and screened patients presenting to MIU, completing preventative onwards signposting and to reduce the number of admissions and community services required in the future.
Project Aims:
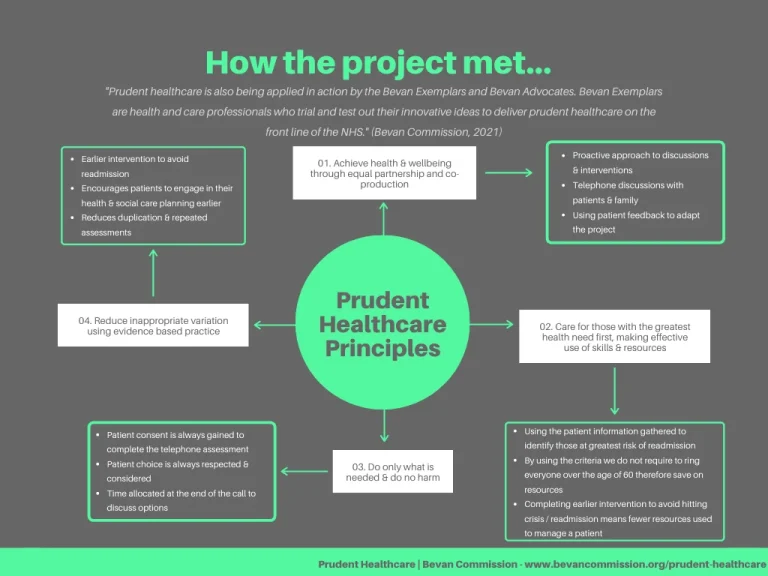
The main aim of the project is to identify key areas of patient needs to reduce the risk of that patient hitting crisis point and re-attending hospital.
Other aims included:
- Setting up a database to capture the screening information gathered and those contacted.
- Forming pathways to ensure consistency with the screening.
- Creating a screening tool to document the information gathered.
- Targeting those over the age of 60 attending MIU with falls, MSK injuries, reduced mobility & head injuries.
- Creating additional links with community services to maintain patients function at home.
- Evaluating data collected to establish the quality and the benefit of the project.
- Obtaining patient feedback comments to ensure benefit from the service user perspective.
Overcoming Challenges:
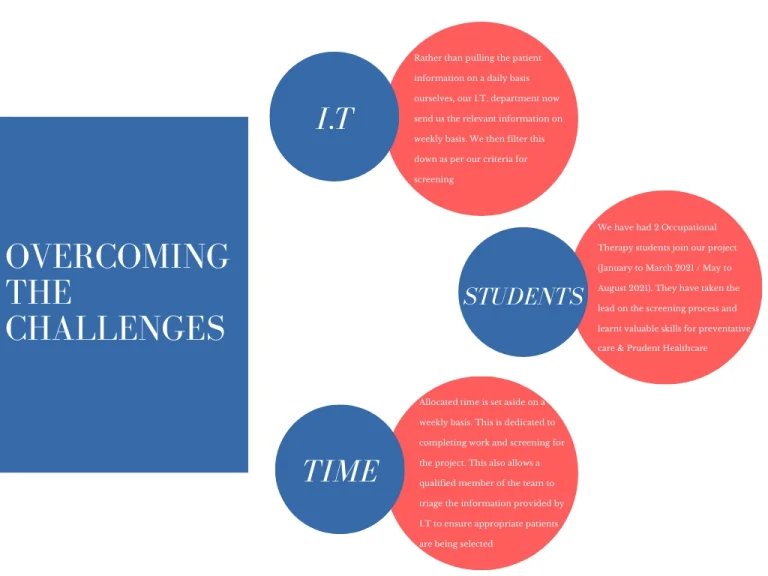
The main challenge of implementing this project has been continuously adapting the service as the demands of the hospital changed due to the pandemic progressing and altering. At the beginning of the project there was ample time to set aside time to gather data and complete telephone calls.
By November 2020, with the second wave hitting the country, workload within the hospital increased and there was less time to complete the screening. Due to lockdown, the patients that are now presenting to hospital are more complex in regards to their functional and social needs and are therefore taking up more clinical time. We have developed strategies to overcome time restraints and these include…
Key Outcomes:
The main key outcome established from the data collected within the project demonstrates a significant increase in number of people assessed. This results in an increase of those in which the service is reaching. The total number of patients screened to date is 441.
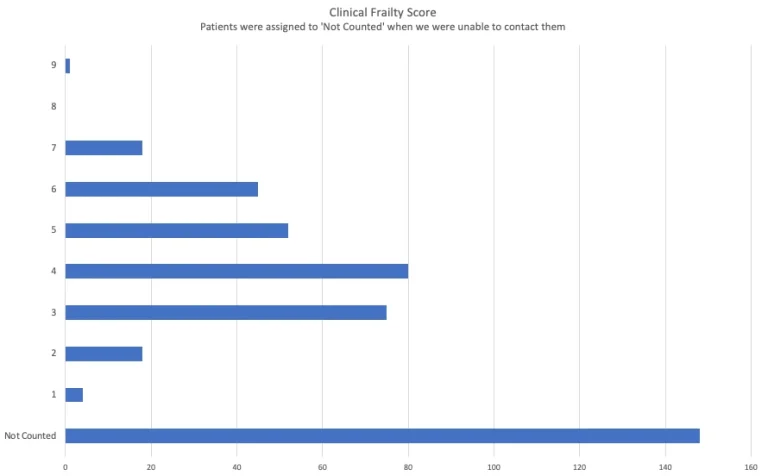
*Although this states “not counted”, these patients were still sent a letter containing the Delta Wellbeing number should they need support in the community.
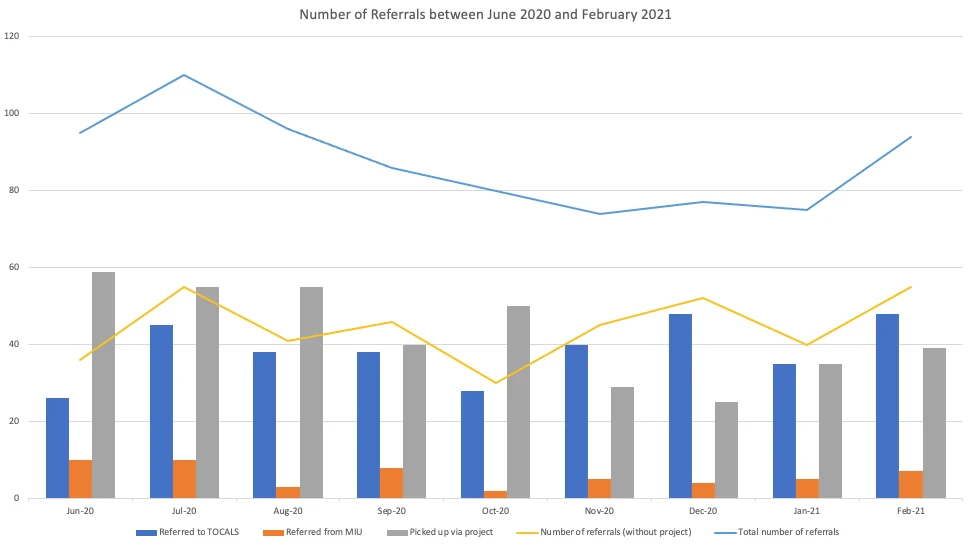
Within 9 months of beginning the project there was an average of 49 patients screened and saw an average increase of 43 referrals per month, ranging from an additional 25 to 59 referrals compared to our standard service (see graph below).
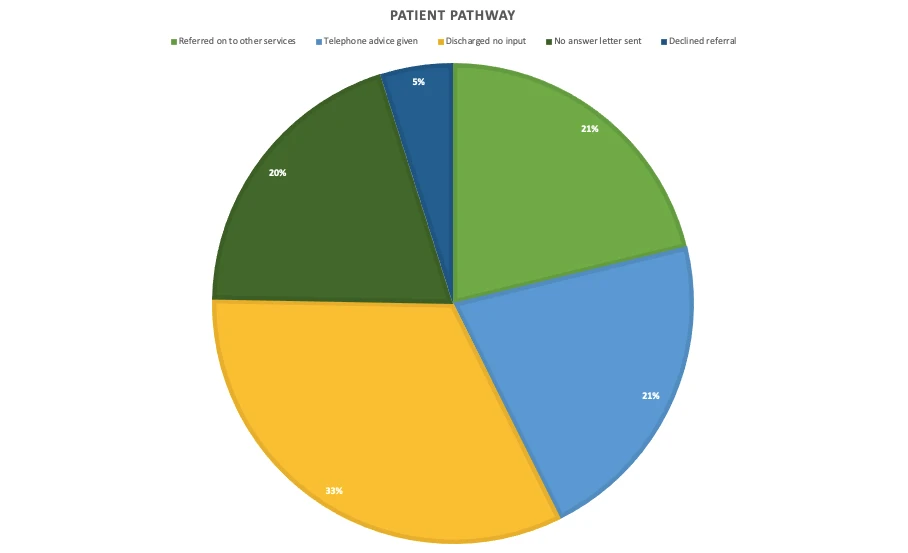
From the data collected we were able to demonstrate that 204 of the patient’s being screened required at least a referral onwards, telephone advice or needs were identified but the patient declined a referral.
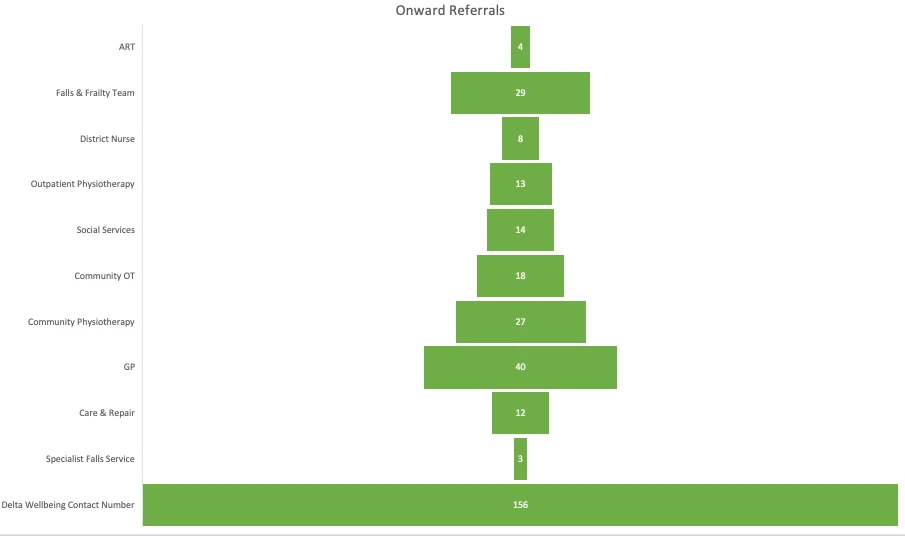
The top three community services that patients were directed back to was Delta Wellbeing, General Practitioners and the Carmarthenshire Community Falls & Frailty team.
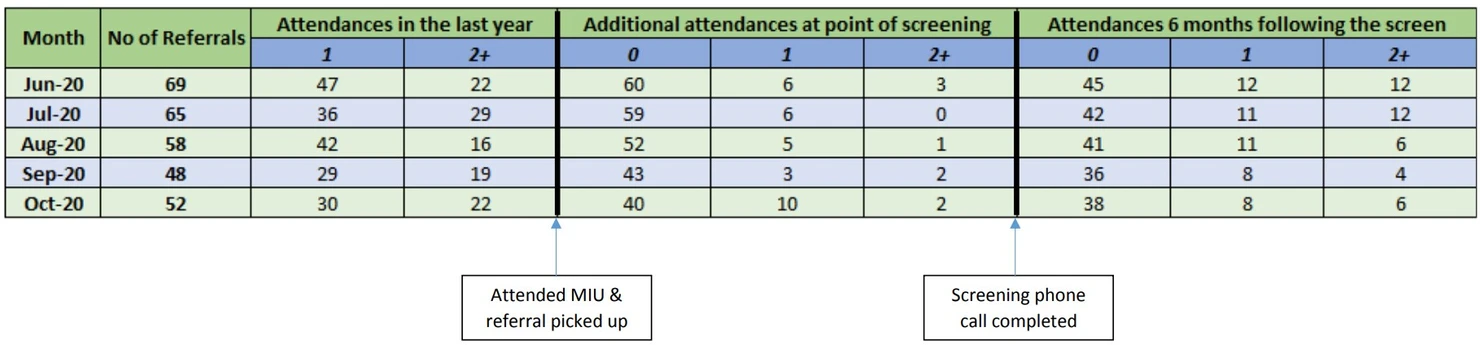
Prior to the screening project patients we identified were also at times frequently attending MIU. We have begun to collect data to demonstrate the impact of the screening on readmission rates 6 months following the initial MIU attendance.
Next Steps:
To conclude I feel this project has demonstrated a need to switch focus to preventative care rather than the current model of reactive interventions. The COVID pandemic has created a significant increase in loneliness within the community and those attending emergency departments are now presenting with increased social care needs.
We have already targeted a significant amount of patients in our local area and provided them with not only advice and support but a friendly phone call to let them know that there are people in their community who can help them. By continuing the screening we hope to reach more of those that require support, to complete low level interventions and sign posting to continue to prevent crisis’ in the community and future admissions.
My Exemplar Experience:
Although initially I was a little apprehensive, my Bevan Exemplar experience has been an incredibly positive and beneficial journey in developing my skills as a clinician. I feel fortunate to have been given the opportunity to explore the service development side of this project through the Exemplar project and I feel that I have taken something new away from every session I have attended. It has been a great experience to network with others who are developing other projects within Wales and I hope to maintain these links into the future. I would recommend anyone considering this path to take the leap and become part of the Bevan Exemplar family.
Showcase:
With thanks to:
Carol-Anne Davies (Service Lead for Acute Occupational Therapists in Carmarthenshire) Aysha Davies (Senior Nurse Manager for Hospital Flow)
Contact:
Carly Pridmore: carly.pridmore@wales.nhs.uk

