Katie Evans and Lee Griffiths
Cardiff and Vale University Health Board
Background
Clozapine, the gold standard for treatment-resistant schizophrenia, carries significant risks. Clozapine-Induced Gastrointestinal Hypomotility (CIGH) affects up to 75% of patients, ranging from mild symptoms (e.g., reflux) to severe, potentially fatal complications (e.g., ileus, obstruction, perforation). Severity relates to clozapine’s pharmacology and patient risk factors.
Screening relies on patient-reported outcomes but lacks detection sensitivity. Given CIGH’s prevalence and detection challenges, prophylactic laxatives have been recommended. A New Zealand protocol reduced serious CIGH cases from 8.2 to 1.1 per 100 person-years (RR 0.13; 95% CI 0.403–0.043).
In 2020/21, CAVUHB implemented a Clozapine Laxative Prophylaxis Pathway (CLPP) for all clozapine patients. This project evaluates CLPP and explores an all-Wales protocol.
Objectives and Approach
1.Evaluate CLPP Uptake: Audit laxative prescribing in CAV clozapine outpatients.
2. Gather Feedback: Survey patients, prescribers & clinic staff on CIGH awareness and CLPP
3. Assess Impact & Value: Review CIGH-related A&E visits/admissions (2006–2025) and cost-benefit of prophylaxis.
4. Map Wales Practices: Identify CIGH prevention approaches & clozapine patient numbers across Health Boards.
Outcomes
-
CLPP Uptake:
Audited 245 clozapine patients.
- 67% prescribed prophylactic laxatives
- Most regimens appropriate
- 15% involved inappropriate polypharmacy
- 1% (n=2) included harmful laxatives
2. Patient and Carer Feedback
- 43% participated; 50% experienced clozapine-induced constipation
- 93% recognised CIGH as serious & supported prophylactic laxatives. Most seek help via clozapine clinic; others turn to family or GPs. Embarrassment limits discussion in clinic.

3. General Staff Knowledge & Feedback
- 89 prescribers responded
- 52% knew of CIGH; 59% of these knew CLPP → greater confidence in CIGH management
- 0% opposed prophylactic laxatives; 49% had reservations or felt it extended beyond their role remit
- Support for CLPP higher among those aware of detection challenges; 50% of uncertain respondents cited outdated “cathartic colon” concerns
“I don’t prescribe Clozapine. I don’t see patients regarding mental health issues”
General Practice prescriber
4. Specialist Staff Knowledge & Feedback
- 13 clozapine clinic staff responded
- 100% aware of CLPP; Reliance on medic prescribing highlighted as timely treatment barrier
- 70% unaware of detection sensitivity & silent nature of CIGH. 61% wanted training to boost confidence in CIGH identification & management
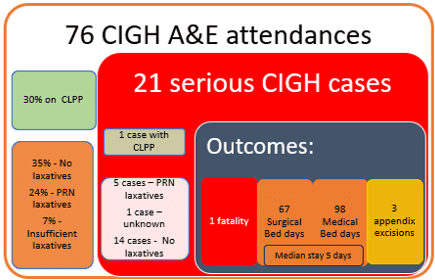
5. Assessing Impact and Value
2103 A&E attendances (355 patients) screened for serious CIGH.
Cost benefit model assumptions:
- Serious CIGH prevalence (literature)
- Current CAV clozapine population
- Maximal CLPP costs
- A&E attendance + 5-day admission (median) + initial investigations
Acute interventions excluded.

6. Practices Across Wales
- 1,685 NHS Clozapine patients
- CIGH prevention practices are variable with inconsistent approaches to laxative prophylaxis
- Laxative prophylaxis could reduce serious CIGH episodes from 138 to 19 per annum
Conclusion
CLPP reduces serious CIGH cases & associated healthcare costs.



