Helen Fitzpatrick and Susan Wynne
Betsi Cadwaladr University Health Board
Rationale for Service Re-design:
In 2012 CAMHS was affected by long waiting times for
routine assessment in excess of 12 months. This was having a negative impact on the quality of service user experience and affecting morale of the clinicians.
There was an acceptance and willingness for change across the teams to alter our methods of service delivery. The CAPA model was proposed as a basis for a re-design of the service.
At that stage there was partially implemented job planning and limited knowledge of skill mix and a lack of clarity about service capacity. We needed a language with which we could describe the amount of work it was possible for the teams to deliver whilst being able to communicate to our organisation what was needed in order to reduce waiting times.
The complex processes involved in our CAMHS needed a framework to examine, streamline and refine systems.
What is CAPA?
CAPA is an evidence based framework for the delivery of modern CAMHS which places emphasis on collaboration and shared decision making with service users (York and Kingsbury, 2013). This model has been adopted by more than 500 services across the UK and the world but has not been widely adopted in Wales.
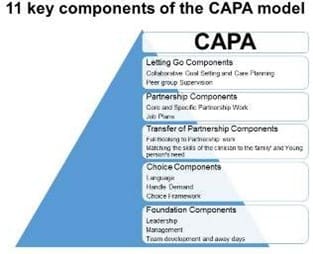
The CAPA model involves several key components and is most effective when all components are in place. It is underpinned by principles of empowerment of children and families to take an active role in improvement of their mental health. It combines demand and capacity theory, evidence based practice, clinical leadership and staff development.
- “Choice” appointments put the service user at the centre of The clinician acts as a “facilitator with expertise” rather than an “expert with power”.
- Work carried out by the team is categorised as “Core” and “Specific” Partnership work – identifying the team skills required to meet the needs of the service users.
- Job planning allows calculation of the availability capacity of a particular skill set.
- Peer group meetings- discussion of the service user goals, any obstacles can be identified or This allows us to learn from each other and facilitates “letting go” of families.
What did we do?
- Consultation with key stakeholders including the service users and the clinicians.
- Training of Clinicians with workshops lead by the originators of the model.
- Put in place the Choice and Partnership system of appointments.
- Set up Peer case discussions.
- Job Planning.
- Regular team away days.
- Regular management meetings to discuss CAPA implementation and review our progress.
What difference does CAPA make?
- Flexible use of capacity to meet We can estimate when demand outstrips capacity and can have a language to describe and a mechanism to evidence this.
- Defining and ensuring provision of functions such as early intervention matched to the needs of the service user with the aim of delivering the right intervention at the right time to the right children, young people and families.
- Collaborative goal setting and care planning with the service user at the centre.
- Collaboration as a vehicle for co-production to enrich service developments.
- Team and individual job plans which define capacity and protect staff from overworking.
- Defined care pathways for major conditions.
Progress to Date and the Future:
All clinicians on the teams now have regular job planning and we have individual and team job plans which can be adjusted according to the demands on the service. We routinely review performance data and activity figures about referrals, choice and partnership activity.
We are using the CAPA framework to deploy new funding from the Welsh Government and have reduced our waiting times to 28 days for routine assessments.
Recruiting skilled CAMHS clinicians is a challenge and we will need to identify and address gaps in the skills of the current workforce.
CAPA processes are part of our induction for new recruits to the service.
In 2012, we were 50% adherent to the model using the CAPA component rating scale. We are currently 77% adherent. We need to be closer to 85%. In order to achieve this we need to further develop our understanding of “core” and “specific” work as well as to promote goal setting by clinicians. To this end we will form a CAPA implementation group the members of which will be drawn from clinicians across the teams.
A further training event is planned for the clinicians and administrations teams to develop an understanding of CAPA.
Planning is underway for CAPA to be introduced in the East and West CAMHS of North Wales and the clinicians from Central area will be experienced and helpful facilitators.
CAPA is Prudent Healthcare:
Public and professionals are equal partners through co-production
CAPA involves the service user in decision making with a clinician whose skills are matched to their needs. The service user is an active participant in their healthcare.
Care for those with greatest healthcare need first, making most effective use of all skills and resources
CAPA model allows for flexible deployment of resource to meet demands with systems that allow for delivery of early intervention.
Do only what is needed no more and no less. Do no harm.
CAPA is a “Pull System” rather than a “push system”. This means that approaches are tailored to the goals of the service user so that no more than necessary is done with a range of flexibly applied approaches.
Reduce inappropriate variation using evidence based practices consistently and transparently. CAPA avoids unnecessary duplication and variation by development of evidence based “care bundles”.
References
York, A. and Kingsbury, S. (2012) The Choice and Partnership Approach. A service Transformation Model. Exeter: Short Run Press.

